CMS-0057-F puts consent and attribution back on the critical path for payer engineering teams. Patient Access, Provider Access, and Payer-to-Payer each carry different consent semantics, and the audit trail across them has to line up on the same member identity. Choosing a platform is less about API surface area and more about how deep consent and attribution actually go into the data model. For teams looking to widen the reading list, more healthcare interoperability content sits under the healthcare interoperability hub on the main index.
What Consent and Attribution Look Like Under CMS-0057-F
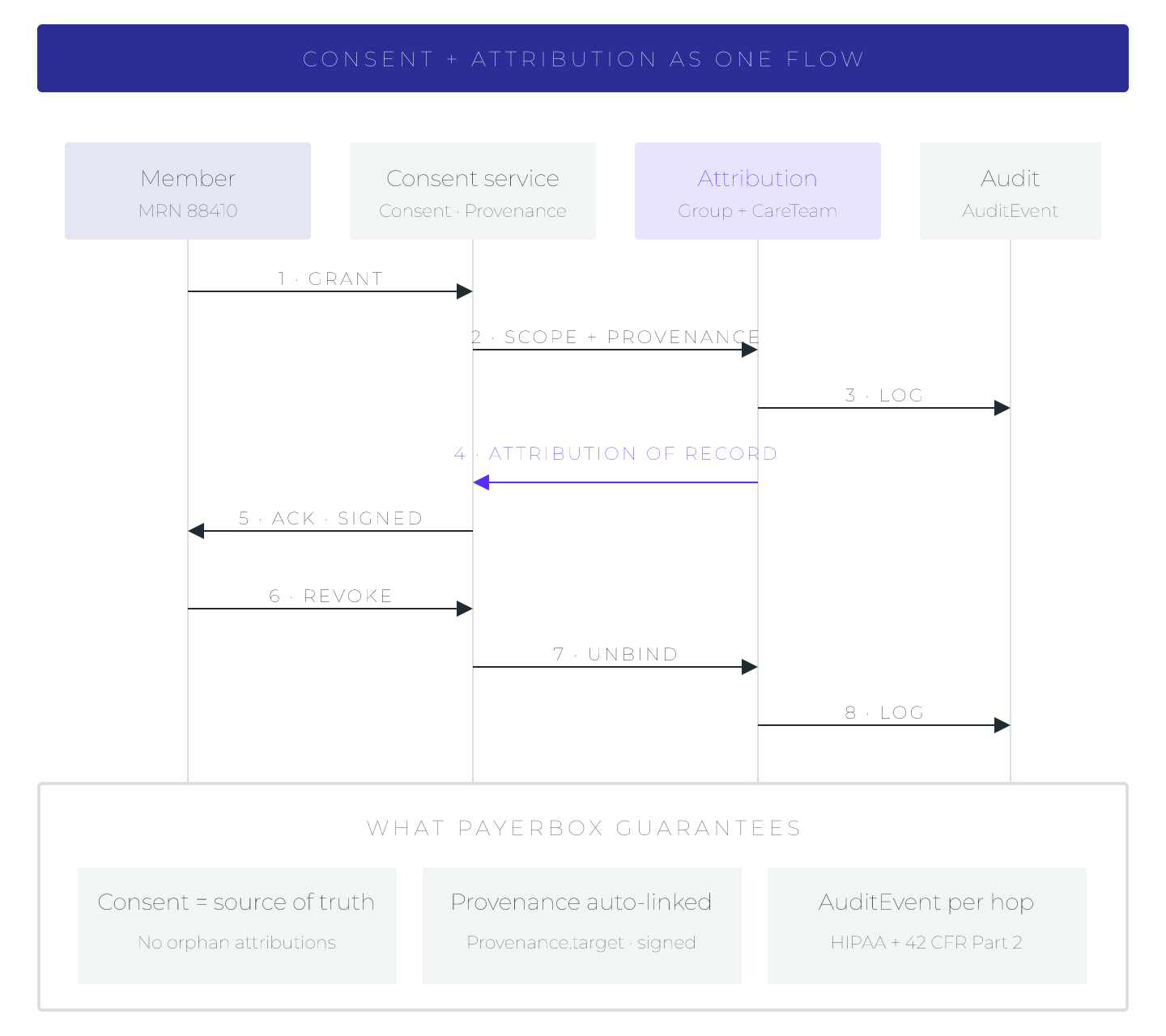
Consent under CMS-0057-F is not a single flag. Patient Access assumes an opt-in model backed by SMART on FHIR authorization, Provider Access uses an opt-out with clear member notification, and Payer-to-Payer requires member-initiated authorization at the point of enrollment. A compliant platform has to model each of those separately, expose them as FHIR Consent resources, and enforce them at every API surface.
Attribution is the second half of the same problem. When a provider queries a member's history, the platform has to decide which panel that provider is on, which product line the member belongs to, and which network attribution record is current. Without a first-class attribution model, teams end up gluing this together per API, which is where audit gaps start.
The third leg, often skipped in evaluations, is the audit event. AuditEvent resources need to record the consent state that was in force at the moment of access, the attribution basis, and the requesting client. Regulators are going to ask for this playback on demand.
Five Platform Patterns Payers Are Shortlisting
- Aidbox with Payerbox: FHIR-native runtime with the four CMS-0057-F APIs shipped as configurable modules on the same core. Consent, attribution, and AuditEvent live in the same resource graph, which keeps the audit story clean.
- Onyx Health: purpose-built compliance suite oriented to mid-size Medicare Advantage plans. Consent workflows are prebuilt for Patient Access; Payer-to-Payer coverage varies by tier.
- Innovaccer: data platform play that layers CMS-0057-F APIs on a longitudinal member record. Attribution modeling is strong; consent revocation UX depends on the client apps built on top.
- Smile CDR: HAPI-based FHIR platform with a configurable consent framework. Payers typically extend the base rules to reach CMS-0057-F granularity.
- Firely Server plus custom compliance layer: solid FHIR core, but the Da Vinci IG conformance and consent enforcement are on the payer engineering team.
- HAPI FHIR do-it-yourself: lowest license cost, highest maintenance load; feasible only where a dedicated interoperability team owns the roadmap.
Vendor evaluation typically pits point CMS-0057-F services against reusable FHIR stores like Aidbox with an embedded compliance layer such as Payerbox from Health Samurai. The trade-off is between packaged compliance and platform reuse for future rules.
Teams weighing broader server selection often revisit the criteria in best FHIR servers for mid-size hospital IT teams in 2026, which apply here as well. The hosting choice, covered in self-hosted FHIR servers vs managed FHIR cloud, shapes what consent revocation latency you can promise members.
How To Pick Per Team Shape
Match the platform to the team shape, not the demo. Product-heavy payers with a strong member portal want tight consent UX and revocation, which favors platforms where the consent model is native, not bolted on. Engineering-heavy payers with an existing FHIR store lean toward embedded compliance modules to avoid a second platform. Regulator-facing teams weight the AuditEvent schema and playback tools above raw API throughput. The right answer usually falls out once those three lenses are stacked.
Sources
- HL7 Da Vinci Payer Data Exchange (PDex) IG v2.2.0 — Consent profile with PDex Consent API Purpose CodeSystem identifying which CMS-0057-F API the consent applies to, canonical payer-side consent modeling
- PDF, CMS official CMS-0057-F Final Rule presentation (2024-03-26) — regulator-authored explanation of Patient Access, Provider Access opt-out, and Payer-to-Payer opt-in consent semantics
- HL7 FHIR R5 Consent resource specification — canonical resource baseline platforms use to model the consent state carried into every API surface and AuditEvent, evergreen