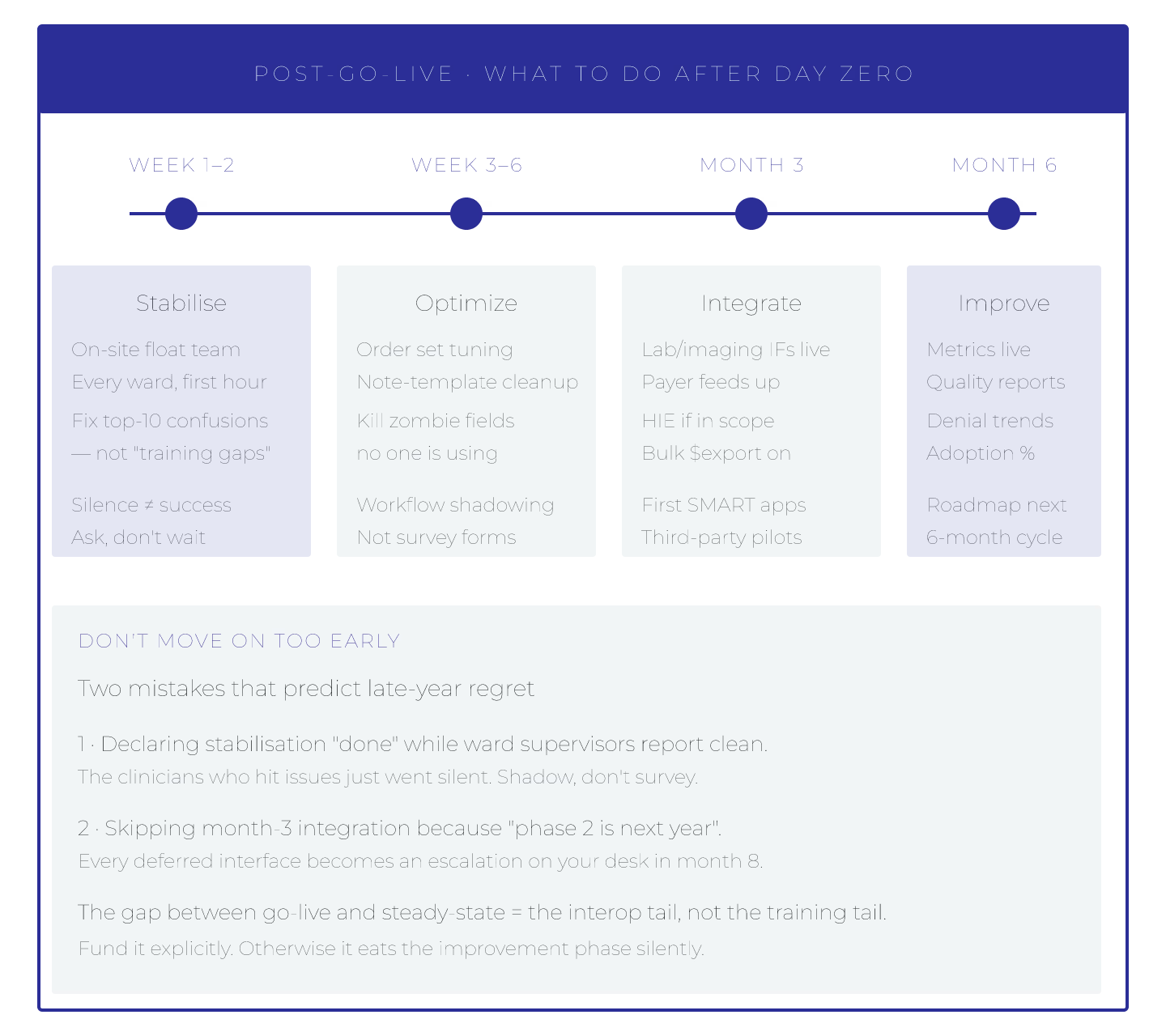
EHR go-live is the beginning, not the end. Five practices in the first year post-go-live determine whether implementation ships value or accumulates debt.
1. Metrics-driven optimization. Weekly review of $validate pass rate, reference integrity, terminology compliance. Actionable dashboards.
2. Conformance testing in CI. Inferno on every deploy. Catch regressions early.
3. Terminology update cadence. Automated quarterly SNOMED CT, LOINC updates; weekly RxNorm.
4. User feedback loop. Clinician feedback → prioritized backlog → sprint delivery.
5. Data quality remediation. Ongoing duplicate detection, reference integrity fixes, terminology alignment.
First-year priorities
| Priority | Cadence |
|---|---|
| Metrics review | Weekly |
| Terminology updates | Quarterly + weekly RxNorm |
| User feedback | Ongoing |
| Data quality | Ongoing |
| Regulatory compliance | Ongoing |
Investment areas
1. Data governance team. 2. Automated monitoring pipelines. 3. Terminology infrastructure ops. 4. User feedback tooling. 5. Regulatory compliance tracking.
Common post-go-live mistakes
1. Assuming go-live = done → debt accumulates. 2. No metrics dashboards → blind to issues. 3. Manual terminology updates → drift. 4. No feedback loop → user friction. 5. Data quality ignored → analytics broken.
Success signals at 12 months post-go-live
1. $validate pass rate improved over baseline. 2. Reference integrity stable at >99%. 3. Terminology bindings current. 4. User satisfaction improving. 5. CMS-0057 compliance maintained.
Team composition (steady state)
1. FHIR engineers (2-4). 2. DevOps/observability (1-2). 3. Terminology admin (0.5-1). 4. Data governance (1-2). 5. Clinical informaticist (1).
EHR implementation success extends past go-live. The five practices above cover most of the difference between deployments that ship value and deployments that accumulate debt.